
This article addresses a prescription agent that belongs to a class of drugs acting on vesicular monoamine transport processes used in certain movement disorders. In plain terms, this medication class works by modulating how monoamine neurotransmitters—particularly dopamine—are packaged and released from nerve terminals. That modulation can reduce patterns of excessive involuntary movement in some clinical contexts. Descriptions here focus on pharmacology, clinical considerations, and research evidence rather than on individualized treatment guidance.
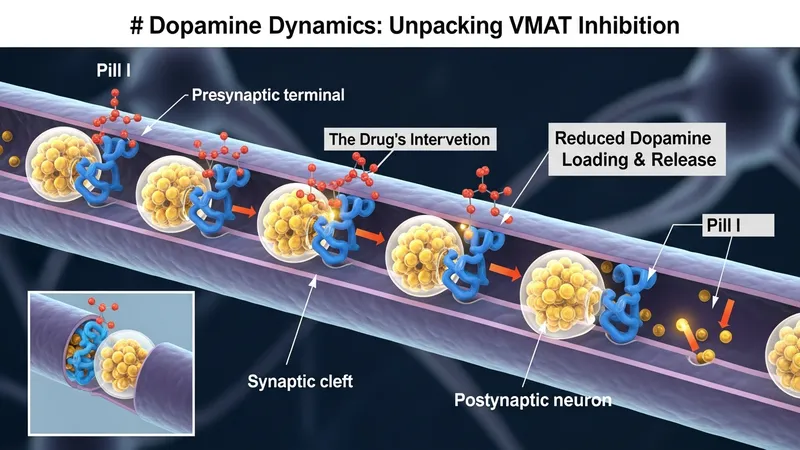
The active approach of this agent involves inhibiting a transporter responsible for loading monoamines into synaptic vesicles. By altering vesicular storage, the amount of neurotransmitter available for release may be reduced, which can change motor signaling patterns in the central nervous system. Pharmacokinetic features such as absorption, hepatic metabolism, and elimination half-life typically influence dosing strategies and monitoring needs. Discussion below stays informational and does not provide medical recommendations.
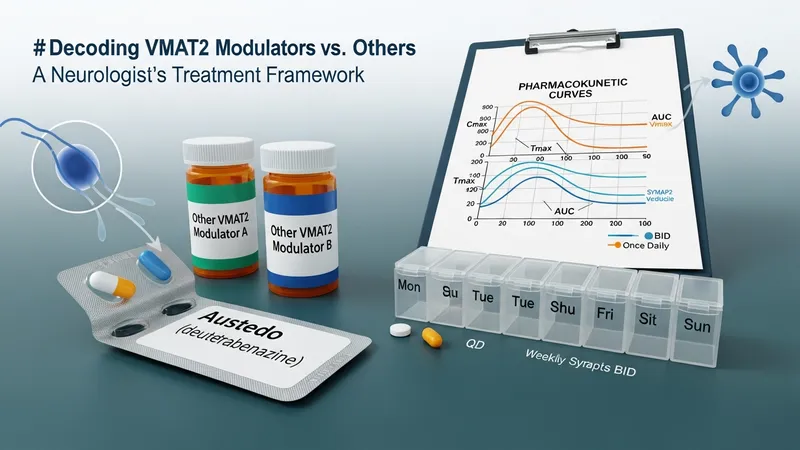
Comparisons among these agents often emphasize differences in metabolism, dosing frequency, and side-effect profiles rather than absolute effectiveness claims. For example, chemical modifications such as deuteration may slow metabolism and can result in altered plasma-concentration-time profiles; this may influence how often doses are given. Clinicians and researchers commonly consider hepatic function, potential for psychiatric adverse effects, and interactions with other drugs that affect monoaminergic systems when evaluating any agent in this class.
Safety considerations typically include monitoring for mood changes, somnolence, and movement-related adverse effects that can arise with modulation of monoamine systems. Laboratory testing is not uniformly required for all patients, but baseline and periodic assessments of liver function may be considered depending on local labeling and clinical context. Drug–drug interactions, especially with medications that inhibit key hepatic enzymes, often inform dose adjustments or selection among alternative agents within this pharmacologic family.
Clinical trial designs for agents in this class frequently use standardized movement scales as primary endpoints, and they often report responder proportions and mean change scores over several weeks to months. Post-marketing surveillance and observational studies can identify rarer adverse events or patterns not fully captured in pre-approval trials. Interpretation of the evidence base may vary by indication, population studied, and trial duration, so systematic reviews and regulatory summaries are commonly consulted for balanced perspectives.
When introducing any of these agents into care discussions, practitioners and researchers typically weigh expected benefits against tolerability and safety considerations in the relevant patient group. Patient-specific factors—such as comorbid psychiatric conditions, hepatic impairment, and concomitant medications—often influence choice among agents that act on vesicular monoamine transport. The next sections examine practical components and considerations in more detail, including mechanism, monitoring, comparative aspects, and research findings.
The principal pharmacologic action of this class involves inhibition of the vesicular monoamine transporter type 2 (VMAT2), which plays a central role in sequestering monoamines into synaptic vesicles. By reducing vesicular uptake, the pool of transmitter available for stimulus-evoked release may be diminished. Dopamine modulation is often the primary focus in movement-disorder contexts, but effects on other monoamines can contribute to clinical and adverse effects. Preclinical and clinical pharmacology reports typically describe concentration-dependent effects and note that central nervous system outcomes arise from altered synaptic monoamine dynamics rather than direct receptor antagonism.
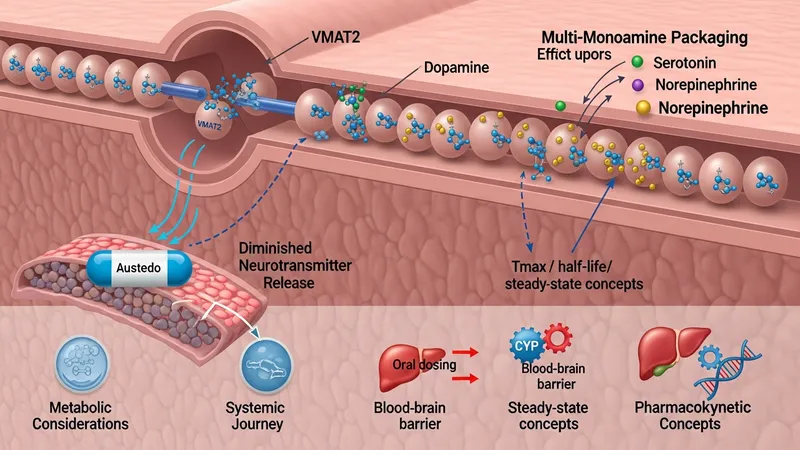
Pharmacokinetic characteristics such as oral bioavailability, time to peak plasma concentration, and half-life influence dosing schedules and steady-state attainment. Some agents in this class have been chemically modified to slow metabolic clearance, which can change exposure variability and dosing frequency. Metabolism is commonly hepatic, involving pathways that may be sensitive to genetic variation and interactions with enzyme inhibitors or inducers. These factors are often documented in regulatory labeling and clinical pharmacology reviews as considerations for clinicians and pharmacologists.
Neurotransmitter interactions relevant to clinical effects include secondary influences on serotonergic and noradrenergic signaling that may occur when vesicular monoamine storage is altered. Such interactions may underlie some psychiatric or autonomic adverse effects observed in trials. Because monoamine homeostasis is complex, investigators often monitor behavioral and affective symptoms in clinical studies and post-marketing settings to detect signals that might warrant additional study or label updates.
Translational research into transporter-targeting agents often includes neuroimaging, neurotransmitter metabolite assays, and electrophysiologic measures to better define mechanism–outcome relationships. These methods can illustrate how modulation of vesicular transport changes circuit-level activity in motor control regions. Readers should note that mechanistic understanding evolves as new studies refine relationships between transporter inhibition, neurotransmitter availability, and clinical manifestations.
Before initiating an agent in this pharmacologic class, clinicians commonly review psychiatric history because mood and behavioral changes have been observed in some patients. Baseline assessments may include mental health screening and evaluation of fall risk or balance issues relevant to movement disorder populations. In practice, liver function tests are often considered when hepatic metabolism is significant, though specific monitoring schedules vary by local guidance and regulatory labeling. Shared decision-making and documentation of baseline status are typically part of a cautious clinical approach.
Monitoring during therapy may focus on emergence or worsening of depressive symptoms, suicidality, excessive sedation, and new or changing movement patterns. Dosing adjustments are sometimes guided by tolerability and clinical response rather than strict laboratory targets. Attention to concomitant medications that affect monoaminergic tone, such as certain antidepressants or antipsychotics, is important because combined effects on neurotransmitter systems can change risk profiles. Pharmacovigilance data and product information usually outline known interactions and monitoring recommendations.
When hepatic impairment or potential drug–drug interactions are present, clinicians and pharmacists often review metabolic pathways and consider alternate regimens or dose modifications described in product information. Genetic variability in drug-metabolizing enzymes can also affect exposure for some agents, and in select cases clinicians may consider this information when available. These considerations aim to balance potential symptomatic benefit against safety and tolerability in the individual patient context.
Informational resources such as regulatory labeling, clinical guidelines, and peer-reviewed reviews commonly provide structured approaches for monitoring and risk mitigation. Those resources may note specific contraindications, recommended baseline evaluations, and thresholds for discontinuation or dose adjustment. In all cases, ongoing surveillance in clinical practice and reporting of suspected adverse events contribute to a more complete understanding of safety profiles over time.
Agents that modulate vesicular monoamine transport are often compared based on pharmacokinetic differences, adverse-effect profiles, and approved indications. For example, some molecules undergo rapid hepatic metabolism and require multiple daily dosing, whereas others with altered metabolic properties may afford less frequent dosing. Comparative discussions in the literature and clinical summaries typically emphasize that selection among agents may be influenced by tolerability, comorbidity profiles, and the specific movement disorder being treated rather than presuming uniform efficacy across all contexts.
Cost considerations and formulary status can influence agent selection in clinical practice, but these factors vary widely across health systems and regions. Economic analyses in published literature sometimes report cost ranges or cost-effectiveness models for different agents, and clinicians may consult formulary guidance when multiple therapeutic options are available. Such practical matters are contextual and do not replace individualized clinical assessment or regulatory labeling for safe use.
Some comparative studies and meta-analyses have examined efficacy outcomes and adverse-effect rates across this pharmacologic family. These analyses often note heterogeneity in study populations, outcome measures, and trial durations, which can limit direct comparability. Researchers and clinicians frequently interpret comparative data cautiously and consider head-to-head trials, observational data, and mechanistic rationale together when discussing how an individual agent may fit into a broader treatment framework.
When transitioning between agents in this pharmacologic group, clinicians typically account for washout periods, overlapping pharmacodynamic effects, and differences in half-life to reduce the risk of additive adverse effects. Practical guidance on switching strategies is often included in specialist guidelines or product documentation and is framed as a clinical consideration rather than a prescriptive instruction, reflecting variability in patient response and clinician judgment.
Clinical trials for transporter-targeting agents commonly use validated movement scales and quality-of-life measures as primary and secondary endpoints. Trial reports often present mean changes from baseline and responder rates at predefined time points. Safety data typically report frequencies of adverse events such as sedation, gastrointestinal symptoms, and neuropsychiatric effects. Post-approval observational studies and registries can supplement trial data by capturing rarer events and longer-term outcomes in broader patient populations.

Signal detection in pharmacovigilance databases can prompt label updates or additional warnings when patterns emerge after wider clinical use. Regulators and independent reviewers analyze such data cautiously, and subsequent studies may be initiated to clarify causality or incidence rates. Research into pharmacogenomics, real-world effectiveness, and long-term safety is ongoing in many centers to better understand individual variability in response and tolerance.
Current research directions include studies of optimal dosing strategies, comparative effectiveness trials, and investigations into mechanisms that underpin differential clinical responses. Preclinical and clinical investigators also examine biomarkers and imaging correlates to refine prediction of benefit and risk. Such work is designed to inform clinical practice by expanding evidence on when and how these agents may be most appropriate for specific patient subgroups.
Overall, the evidence base is iterative: randomized trials provide controlled efficacy and safety data over defined periods, while post-marketing and observational research add complementary information about longer-term use and rarer adverse events. Readers seeking more detail are advised to consult regulatory summaries and peer-reviewed literature for source data and methodological context rather than relying on single reports or anecdotal accounts.