
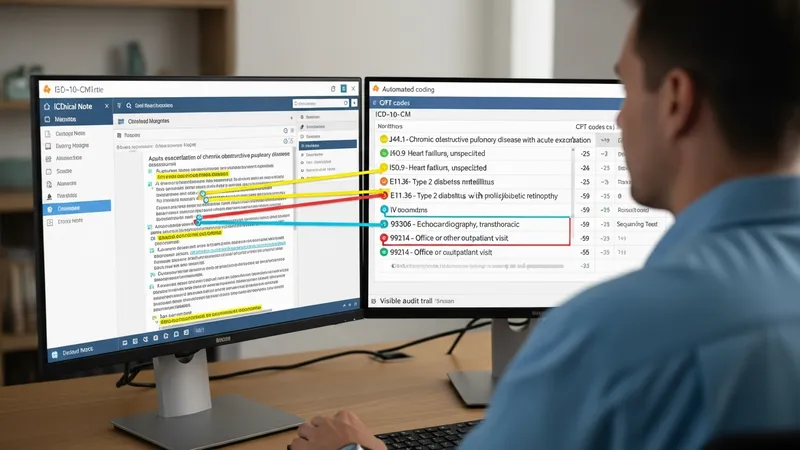
Automated platforms that assist with assigning standardized clinical codes use software to analyze clinical notes, procedure records, and encounter data and suggest appropriate diagnostic and procedure codes. These systems often apply natural language processing (NLP) to extract clinical terms from narrative text, map extracted concepts to code sets such as ICD-10-CM and Current Procedural Terminology (CPT), and present suggested codes for review. In United States clinical settings, the software typically integrates with electronic health records (EHRs) and billing workflows so coding suggestions can align with claims preparation and internal documentation improvement efforts.
Such platforms vary by method and scope: some focus on automated suggestions for common diagnoses, others aim to support inpatient coding, and some include tools for clinical documentation improvement (CDI). Outputs may include suggested codes, confidence scores, links to source text, and audit logs for reviewer actions. Human coders or clinical documentation specialists commonly review and validate suggested codes before submission to payers. The extent of automation and the human review workflow may differ by product and facility size, and each approach may affect coder workload, audit readiness, and claim accuracy in different ways.

Selection criteria for examples above reflect commonly referenced vendors and tools in U.S. healthcare coding discussions and focus on systems that interact with standard U.S. code sets and payer processes. These items were chosen to illustrate different approaches—vendor-provided encoder/reference tools, enterprise coding suites, and documentation-centered solutions—rather than to rank them. Readers should consider compatibility with institutional EHRs, support for ICD-10-CM and CPT, and capacity for human review when comparing systems in United States contexts.
In practice, automated coding systems often rely on NLP pipelines that identify clinical entities, normalize terminology, and map to code concepts. The mapping step may consult code set rules, payer edits, and facility-specific guidelines. NLP performance can vary with documentation style, specialty-specific language, and the quality of structured data inputs. In United States settings, systems that explicitly reference ICD-10-CM and CPT nomenclature and that can surface the originating text segment for reviewer verification may support clearer coder decision-making and defensible audit trails.
Human oversight remains a central element: many organizations use “human-in-the-loop” workflows where suggested codes are reviewed by certified coders or CDI specialists before claim submission. This arrangement can help identify ambiguous documentation, clinical nuances, or coding rules that automated mapping may not reliably capture. Reviewers typically examine confidence indicators, source text highlights, and related clinical fields. The review step also provides feedback loops that may be used to tune system configuration or inform vendor-supported model updates within U.S. compliance frameworks.
Data privacy and regulatory alignment are important considerations in United States deployments. Systems that process protected health information (PHI) must adhere to HIPAA safeguards and institutional policies for data handling. Contracts, Business Associate Agreements, and technical safeguards such as encryption and access controls typically form part of a compliance posture. Additionally, alignment with Centers for Medicare & Medicaid Services (CMS) documentation expectations and audit readiness procedures is often a planning focus when introducing automation into U.S. coding operations.
Operationally, organizations may evaluate automated coding by tracking coder productivity metrics, query volumes for documentation clarification, and claim denial patterns over time. Such measurements may indicate where automation can supplement routine tasks and where manual review continues to be necessary. These evaluations typically use conservative interpretation—automation may influence metrics in measurable ways, but results can vary by specialty mix, documentation practices, and implementation scope. The next sections examine practical components and considerations in more detail.
Automated coding approaches in U.S. clinical environments commonly fall into several categories: rule-based encoders that apply deterministic mapping and payer edit logic; machine learning models that learn associations between text and codes from labeled examples; and hybrid systems that combine rule-based checks with statistical or neural NLP components. Rule-based systems may be predictable for certain mappings and payer rules, while machine learning methods may handle linguistic variability better but often require labeled data and careful validation. Hybrid models are frequently used to balance repeatable rule application with flexible language understanding in United States settings.

Implementation choices often reflect workflow needs: encoder-style tools can be integrated as reference engines within coder workflows, while ML-driven systems may operate as pre-coding assistants that flag likely codes for human review. For inpatient versus outpatient contexts, model training data and rulesets typically differ because ICD-10-CM sequencing, principal diagnosis determination, and procedure coding conventions may vary. Organizations commonly pilot different approaches in controlled areas before broader rollout to evaluate fit with specialty documentation and claims processes.
Model validation and monitoring are practical considerations: in the United States, acceptable performance is often assessed against coder-reviewed gold standards and through ongoing sampling for accuracy and compliance with CMS and payer expectations. Version control for mapping logic and annotation guidelines helps maintain traceability. Additionally, transparency about how a system arrives at a suggestion—such as showing the source sentence and extracted entities—can aid coder acceptance and efficient review within U.S. clinical coding teams.
Operational integration considerations include where in the documentation lifecycle the tool acts (real-time during documentation, post-encounter pre-billing, or retrospective coding audits) and how coders interact with suggested codes. Each mode has trade-offs: real-time suggestions may support documentation completeness but require in-EHR integration, while post-encounter tools may focus on billing accuracy and require strong interfaces with practice management and claims systems in U.S. healthcare organizations. These distinctions help frame pilot design and evaluation.
Automated coding systems in the United States must operate within the framework of national code sets and regulatory guidance. ICD-10-CM is maintained for diagnoses, CPT for procedures and services, and CMS provides payer-specific billing and documentation guidance. Systems that generate code suggestions typically reference current code set versions and implement logic to reflect sequencing rules, modifiers, and documentation requirements. Institutions often align vendor configurations with internal medical record policies and with guidance from CMS or the American Medical Association (AMA) to maintain consistent coding practices.
Audit preparedness and documentation support are common regulatory focal points. U.S. healthcare organizations may face internal audits, payer audits, or Medicare program integrity reviews; maintaining accessible audit trails, source text highlights, and reviewer actions can support responses. Automated systems that preserve evidence of reviewer validation and retain linking between suggested codes and source documentation may assist in demonstrating compliance during reviews. Facilities often establish procedures to reconcile automated suggestions with institutional coding policies and legal obligations under applicable U.S. law.
Privacy and data protection requirements under HIPAA guide how PHI is processed and stored. Business Associate Agreements and technical security measures such as encryption, access control, and logging typically accompany deployments. Where cloud or third-party processing is used, contracts and security assessments often address location of data storage, permitted uses, and incident response expectations consistent with U.S. regulatory requirements. These controls are typically considered during vendor selection and contracting stages to ensure alignment with institutional risk frameworks.
Keeping code sets and guidance current is an ongoing activity: annual and periodic updates to ICD-10-CM and CPT, and to payer policy, can affect automated mappings. U.S. organizations often plan for version updates, testing windows, and change management processes so that system behavior remains aligned with current billing rules and documentation standards. Coordination between clinical, coding, compliance, and IT teams typically supports timely updates and reduces risk of mismatches between clinical documentation and coded output.
Practical integration with electronic health records (EHRs) and revenue-cycle systems is a central implementation challenge in U.S. settings. Many hospitals and ambulatory groups use EHRs from vendors such as Epic or Oracle Cerner; integration points may include direct API connections, HL7 interfaces, or middleware. The choice of integration method can influence latency of suggestions, the location where coders review recommendations, and how documentation edits flow back into the record. Technical compatibility and interface testing are typical early steps in U.S. deployments.
Human collaboration models generally adopt a human-in-the-loop approach where certified coders, clinical documentation improvement specialists, or clinicians validate and finalize codes. Worklists, confidence scoring, and user interfaces that highlight source text are commonly used to support efficient review. In many U.S. organizations, these collaboration features help maintain coder oversight and institutional control over final coding decisions while allowing automation to assist with routine or high-volume mapping tasks.
Change management and training are important operational elements. Staff may need orientation to new user interfaces, to interpretation of confidence indicators, and to procedures for challenging or correcting automated suggestions. U.S. facilities often pilot systems in selected departments to gather feedback and refine workflows. Metrics such as query rates for clarification of documentation, coder throughput, and coding accuracy sampling are commonly tracked to assess impacts and guide iterative improvements without framing automation as a substitute for professional judgment.
Audit trails and reporting capabilities can support governance and continuous improvement. Systems that log suggestion provenance, reviewer actions, and timestamps create records useful for internal quality assurance and for responding to external inquiries. Reporting that summarizes types of suggestion edits, frequent documentation gaps, or specialty-specific patterns may inform targeted education for clinicians and coders. Such analytical outputs are typically used as informational inputs for process refinement rather than as definitive performance guarantees.
Costs for automated coding systems in the United States vary based on deployment model, scale, and feature set. Common cost components include software licensing or subscription fees, implementation and integration services, data migration or configuration fees, and ongoing maintenance or support. Small practices may engage hosted subscription services with lower upfront costs, while larger hospitals often budget for enterprise licensing and more extensive integration. Conservatively, U.S. organizations may encounter annual software and support costs that range from several thousand dollars for small deployments to hundreds of thousands of dollars for enterprise-scale implementations, depending on scope and vendor terms.

Deployment models include cloud-hosted services, on-premises installations, and hybrid approaches. Cloud models can reduce local infrastructure requirements but often involve data-hosting considerations and contractual safeguards under HIPAA; on-premises models may give greater local control at the cost of infrastructure and internal IT responsibilities. Hybrid models may keep PHI on premises while using cloud-based analytics for de-identified telemetry. Choice of model commonly reflects institutional risk tolerance, IT capacity, and regulatory or contractual constraints in the United States.
Evaluation metrics used by U.S. organizations to measure system performance typically include coding suggestion accuracy (measured against coder-reviewed samples), changes in coder throughput, documentation query volumes, and claim denial trends. Financial metrics such as impact on claim rework or denial recovery are sometimes tracked as informational estimates, though organizations usually avoid absolute claims and interpret results in context of specialty mix and documentation practices. Continuous monitoring and periodic audits are typically recommended to detect drift in automated performance over time.
Decision-making commonly involves multidisciplinary stakeholders—coding leadership, compliance, revenue cycle, IT, and clinical representatives—to assess fit and risk. Pilot projects with defined scope and measurable objectives often provide early evidence for whether a given configuration supports institutional goals. Evaluation typically emphasizes transparency about system behavior, ongoing validation against professional coding standards, and alignment with U.S. regulatory requirements rather than promises of fixed outcomes. Overall, careful, measured planning and monitoring are typical practices when U.S. organizations consider automated coding assistance.