
The All-on-4 concept describes a full-arch dental rehabilitation approach that uses a small number of implants to support a fixed prosthesis for an entire dental arch. Rather than replacing each missing tooth individually, clinicians position four implants in strategic locations to maximize use of available bone. Two anterior implants are commonly placed near the midline and two posterior implants are often tilted to engage denser bone and reduce the need for extensive grafting. This approach typically coordinates surgical placement with prosthetic planning so that a provisional prosthesis can be delivered within a short postoperative interval when clinical conditions allow.
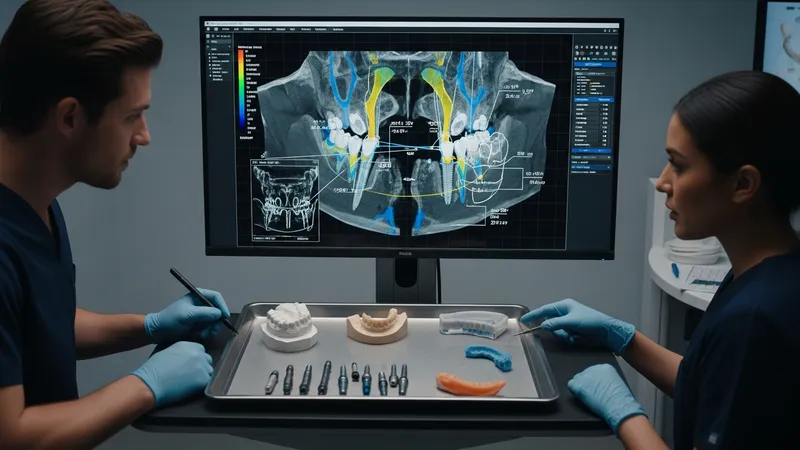
Clinical planning for this full-arch method typically integrates radiographic assessment, implant angulation strategies, and provisional prosthetic design. Cone-beam imaging and digital planning platforms are often used to evaluate bone volume and to design surgical guides when applicable. The treatment sequence can include preparatory extractions, immediate implant placement, and delivery of an interim restoration that permits functional loading of the arch under controlled conditions. Clinicians and dental teams typically discuss case selection criteria, such as bone quality and patient systemic factors, when evaluating suitability for a reduced-implant full-arch plan.

Comparative frameworks often describe the tilted-posterior configuration versus conventional parallel implant placement. The tilted approach may allow longer implant engagement in anterior bone and often reduces the posterior cantilever length of a prosthesis. By contrast, parallel placement can be used when posterior bone volume and anatomy permit. When comparing methods, clinicians typically consider implant angulation, prosthetic connector positions, and occlusal scheme implications. Reports commonly note that choice of approach can influence the need for additional grafting procedures and may affect how soon a provisional prosthesis can be delivered.
Digital tools and guided workflows may improve preoperative visualization and help translate a planned implant trajectory to the clinical field. Computer-guided planning typically uses three-dimensional imaging to assess anatomical limitations and to virtually position implants relative to prosthetic goals. Surgical guides fabricated from that plan can be tooth-, mucosa-, or bone-supported depending on the case. While guides may enhance reproducibility, clinicians often emphasize the importance of intraoperative judgement, as guide deviation and clinical variables can require real-time adjustment.
Immediate provisionalization is a commonly discussed component of this implant approach and is often presented as a way to restore function and esthetics during healing. Provisional prostheses are typically made from acrylic or composite materials and are designed to manage occlusal load while osseointegration progresses. Clinical protocols often define insertion torque or primary stability thresholds that may influence whether immediate provisionalization is attempted. Where immediate loading is not pursued, a removable prosthesis or delayed fixed restoration may be used as an interim option while healing proceeds.
Case selection and interdisciplinary coordination are recurrent themes when planning a reduced-implant full-arch restoration. Patient factors such as smoking, systemic conditions, and oral hygiene can influence treatment timing and maintenance strategies. Additionally, laboratory capabilities and digital workflow maturity may affect prosthetic timelines and the choice between a provisional and a definitive prosthesis. When multiple approaches are available, teams often weigh surgical complexity, prosthetic requirements, and patient-specific anatomic constraints to select an appropriate pathway.
In summary, the full-arch strategy that uses four strategically placed implants offers a framework that integrates implant angulation, guided planning, and provisional prosthetic sequencing. The approach may reduce the need for extensive grafting in certain anatomic situations and often relies on coordinated surgical and prosthetic steps. The next sections examine practical components and considerations in more detail.
Preoperative assessment for a four-implant full-arch solution typically begins with a comprehensive clinical exam and three-dimensional imaging to evaluate bone volume, sinus anatomy, and neurovascular structures. Digital planning software may be used to simulate implant positions and to design provisional prostheses; this often improves visualization of prosthetic emergence profiles. Case records commonly include study models, photographs, and occlusal analysis. When available, multidisciplinary input from restorative dentists and laboratory technicians may refine the prosthetic plan. These planning steps are considered important for matching implant placement to the intended final restoration while accounting for patient-specific anatomy.
Selection of implant positions usually balances prosthetic needs and bone availability. The anterior implants are often placed axially in denser bone, while posterior implants may be tilted to engage additional anteroposterior bone and to reduce posterior cantilever. Tilted placement can reduce the need for grafting in some jaws, although clinicians typically evaluate sinus proximity and bone angulation carefully. Planning may also consider implant diameter and length choices that correspond to primary stability expectations and prosthetic connector positions used in later prosthesis fabrication.
When computer-guided planning is used, surgical guides can be fabricated to transfer the virtual plan to the surgical field. Guides may be tooth- or mucosa-supported depending on whether teeth remain and on soft tissue conditions. Guided placement may assist in achieving intended angulation and depth, yet clinicians usually allow for intraoperative verification and potential deviations. Accuracy of guided systems can vary and is influenced by imaging quality, guide seating, and the surgical protocol; thus, guided workflows are presented as tools to enhance, not replace, clinical judgment.
Preoperative communication with the dental laboratory regarding provisional design often shapes immediate postoperative expectations. Provisional restorations that are fabricated in advance or milled after planning can be adjusted chairside and are typically designed to control occlusal forces during the initial healing phase. In addition, patient counseling about maintenance needs and realistic timelines for definitive prostheses is commonly discussed. These planning and assessment steps aim to align surgical positioning, provisional prosthetic function, and long-term restorative goals.
Surgical sequencing commonly starts with atraumatic extractions when necessary, followed by alveolar debridement and assessment of implant bed conditions. Flap design choices may vary; some clinicians prefer a limited flap while others use full access depending on anatomic considerations. Drilling sequences and osteotomy depth are guided by preoperative planning; primary stability metrics such as insertion torque or implant stability quotient (ISQ) readings are often monitored intraoperatively. These metrics may inform decisions on immediate provisionalization, with teams typically setting conservative thresholds rather than absolute values.
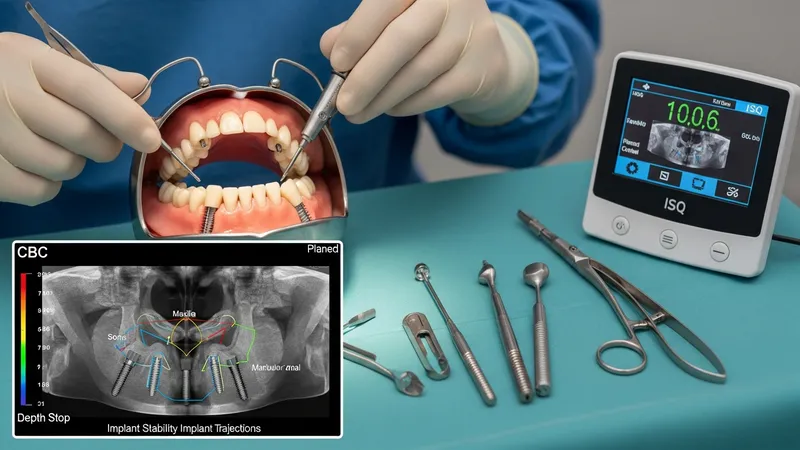
Tilted posterior implant placement requires attention to angulation and emergence relative to the prosthesis. When posterior implants are angled, components and prosthetic abutments are selected to correct prosthetic emergence and to orient screw access favorably. Tilted implants may engage denser cortical bone anteriorly, which can enhance primary stability in some cases. However, clinicians must assess individual anatomy—sinus locations, mandibular canal position, and ridge morphology—to avoid encroachment on critical structures while achieving the planned trajectory.
Computer-guided surgery can be integrated with the operative steps to transfer the planned implant positions to the mouth. Guide-supported osteotomies are typically executed with long drills and guide sleeves, and clinicians often verify guide fit prior to preparation. In freehand placement, planned angles are translated using surgical stents or reference points from the plan. Whichever approach is used, surgeons commonly confirm prosthetic component compatibility intraoperatively and adjust for passive fit to reduce prosthetic stress at the time of loading.
Immediate provisional delivery is a step that often follows implant placement when primary stability thresholds are met. Temporary fixed prostheses are usually designed to control occlusal contacts and to minimize lateral loading during healing. Where immediate loading is not appropriate due to insufficient stability or unfavorable tissue conditions, clinicians may opt for a nonfunctional interim solution and plan definitive restoration after osseointegration. Postoperative protocols commonly include medication management, dietary recommendations, and scheduled follow-up to monitor healing and prosthesis function.
Prosthetic options for a four-implant full-arch solution often include an interim removable or fixed prosthesis followed by a definitive fixed restoration. Interim prostheses are frequently fabricated from acrylic or composite materials and are used to evaluate esthetics, speech, and occlusal schemes while the implants integrate. Definitive prostheses can be constructed using layered acrylic over a metal framework, composite on titanium frameworks, or monolithic zirconia hybrids depending on laboratory capabilities and patient needs. Material selection typically balances durability, reparability, esthetics, and occlusal load considerations.

Framework design and connector position are essential for achieving passive fit and even load distribution across implants. Frameworks may be milled from titanium or other surgical alloys to provide a rigid substructure that resists deformation under function. Prosthetic screw access channels are planned to avoid occlusal table interference when possible, and angled abutment components can be used to correct screw access orientation for tilted implants. Lab communication and digital design files are often used to verify fit before final insertion.
Occlusal scheme choices for definitive restorations commonly aim to reduce lateral forces and to promote axial load distribution across implants. Clinicians often use mutually protected occlusion or other schemes adjusted to the prosthesis design and opposing dentition. Nighttime bruxism considerations may influence material choice or the recommendation of occlusal appliances as a management strategy. Prosthetic maintenance planning, such as scheduled screw checks and hygiene instruction, is typically incorporated into the restorative timeline.
Digital workflows that combine intraoral scanning, CAD/CAM design, and laboratory milling have become more common in prosthetic fabrication. Digital impressions can capture implant positions via scan bodies and facilitate design iterations prior to milling or 3D printing. These workflows may reduce turnaround time for definitive prostheses and allow for better reproducibility of the planned emergence profiles and occlusal schemes. However, clinicians usually evaluate digital accuracy on a case-by-case basis and maintain quality checks during laboratory steps.
Postoperative follow-up typically includes scheduled clinical reviews to monitor soft tissue healing, prosthesis function, and peri-implant conditions. Maintenance protocols commonly recommend regular professional evaluations that may include radiographic assessments to track marginal bone levels and to detect early peri-implant changes. Oral hygiene training and adjunctive tools such as interdental brushes or water irrigation devices are often discussed to help patients maintain implant and prosthesis longevity. Long-term maintenance is framed as a collaborative effort between the clinician, laboratory, and patient.

Management of complications is approached as part of standard clinical practice; clinicians may monitor for signs of prosthetic screw loosening, occlusal wear, or soft tissue inflammation and address them through adjustment, repair, or additional interventions as indicated. Where peri-implant mucositis or peri-implantitis is suspected, non-surgical and surgical management strategies may be considered based on clinical findings. These management pathways are typically individualized and may involve both restorative and surgical disciplines to optimize outcomes.
Reported implant survival and prosthesis success in the literature vary by study design and follow-up period; many cohort reports and systematic reviews describe survival rates that in some settings commonly exceed 90% over five to ten years, while acknowledging variability across patient populations and protocols. Such figures are often presented as general observations rather than guarantees, and clinicians usually interpret published outcomes in the context of patient-specific factors, surgical technique, and prosthetic maintenance practices.
Long-term considerations also include planning for prosthesis repair or replacement over time, as materials can wear and screw-retained connections may require periodic maintenance. Patient education about dietary habits, parafunctional habits, and signs that warrant prompt assessment is commonly provided. Future follow-up sections and case reviews often focus on maintenance regimens, realistic timelines for prosthetic refurbishment, and strategies to monitor peri-implant health while adapting care to individual clinical courses.