
When a person and a clinician explore prescription options to support body-weight management, the conversation typically covers medication types, how those treatments work, and the practical steps for safe use. This process involves reviewing medical history, discussing goals and expectations, and considering non-pharmacologic supports such as nutrition and activity. The focus is on informing both patient and clinician so they can weigh potential advantages and risks together rather than making unilateral decisions.
Such discussions often examine eligibility criteria, available formulations, expected courses of treatment, and monitoring needs. Clinicians may describe mechanisms of action, common dosing schedules, likely side effects, and how medications may interact with other conditions or treatments. The exchange is factual and individualized: it aims to clarify what different options involve and what follow-up might be needed to assess effectiveness and tolerability.

Comparing medication classes and mechanisms may help a clinician and patient identify which options align with the patient's clinical profile. Mechanisms that act on appetite centers or gastrointestinal signaling can affect hunger cues, satiety, and caloric intake in different ways. Differences in pharmacokinetics—such as weekly versus daily dosing—can influence adherence patterns and monitoring plans. These distinctions are presented as factual differences rather than value judgments, and they may shape a care plan depending on patient preference, coexisting conditions, and tolerability.
Eligibility and screening typically form the early part of a clinical discussion. Clinicians often review current medications, medical comorbidities such as pancreatic or thyroid conditions, pregnancy potential, and prior treatment history. Laboratory testing and vital-sign assessment may be suggested to establish baseline status. These steps are intended to identify contraindications or precautions and to inform a monitoring schedule; they do not imply a prescriptive outcome but rather support clinical judgment and patient safety during follow-up.
Dosing, titration, and monitoring commonly become practical points of focus. Many regimens begin at a lower dose with gradual increases to reduce side effects. Clinicians often explain typical adjustment timelines and common adverse effects such as gastrointestinal symptoms, and they outline when to seek medical review. The aim is to provide realistic expectations about the initiation period and what kinds of transient effects may occur, emphasizing surveillance rather than promising specific results.
Integration with behavioral and lifestyle approaches is usually part of an evidence-informed plan. Medication is often discussed as one component among dietary, physical activity, and behavioral counseling strategies. Multidisciplinary support—nutrition counseling, physical-activity planning, or behavioral therapy—may be described as complementary rather than required. Clinicians typically frame these components as ways to support sustainable changes while monitoring how medication and lifestyle adjustments interact over time.
In summary, clinical conversations about prescription medications for body-weight management are structured to clarify options, screening needs, and monitoring plans while placing medication in the context of broader care. The goal of such discussions is to equip the patient and clinician with information to make reasoned, individualized decisions about whether and how to proceed. The next sections examine practical components and considerations in more detail.
Understanding pharmacologic classes helps frame clinical choices. GLP-1 receptor agonists act on receptors that influence appetite, gastric emptying, and insulin secretion, whereas dual GLP-1/GIP agonists engage additional pathways tied to metabolic regulation. Differences in molecular structure and receptor activity can produce varied efficacy and tolerability profiles. When clinicians explain mechanisms, they often focus on how a drug is taken (oral or injectable), how often it is dosed, and which physiologic pathways it most directly affects. These factors may guide considerations about suitability for a particular patient.
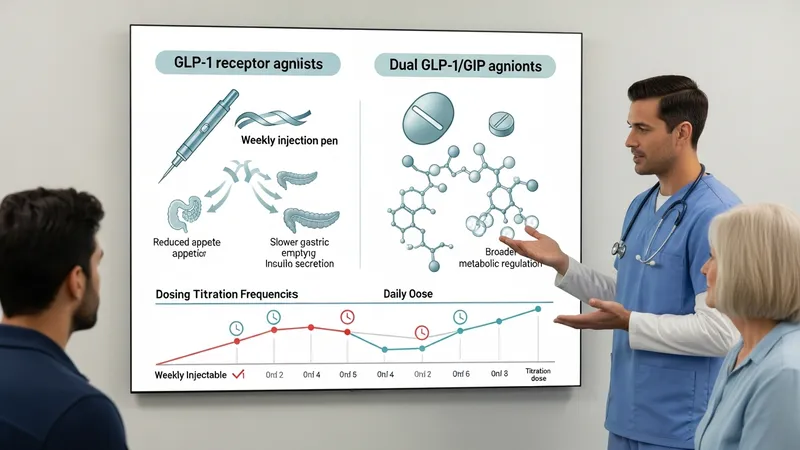
Comparative aspects that may factor into selection include onset of action, typical titration timelines, and administration route. Weekly injectables can reduce exposure to daily dosing decisions, while daily options may allow more rapid dose adjustments. Clinicians sometimes discuss how pharmacokinetic properties relate to side-effect timing and the convenience of administration. This technical information is presented so patients can consider practical implications alongside clinical suitability rather than as prescriptive advice.
Evidence summaries and guideline excerpts commonly referenced in clinical settings often describe relative benefits, limitations, and safety signals for different classes. Such summaries typically report average ranges of weight change observed in trials and common adverse effects, but clinicians emphasize individual variation. In practice, clinicians may frame trial outcomes as context rather than guarantees, noting that real-world responses can differ and that ongoing monitoring is required to assess individual response and tolerability.
When discussing mechanisms, clinicians may also highlight interactions with other treatments or conditions. For example, agents that slow gastric emptying can affect oral medication absorption, and some therapies have contraindications in certain gastrointestinal or endocrine disorders. These interaction points are discussed as safety considerations and may prompt alternative strategies or closer follow-up rather than an immediate exclusion from treatment.
Initial clinical assessment commonly includes medical history, physical examination, and targeted laboratory testing. Baseline evaluation may review cardiovascular risk factors, glycemic status, liver and kidney function, and potential contraindications. Reproductive plans and pregnancy testing may be discussed when relevant, since some agents require avoidance during pregnancy. The intention of baseline screening is to identify conditions that would alter risk–benefit considerations or necessitate an alternative approach.

Clinicians often use standardized criteria and clinical judgment to determine candidacy for medication. These criteria typically combine measures such as body-mass index, presence of weight-related comorbidities, and prior response to lifestyle interventions. That said, exact thresholds and eligibility frameworks can vary by guideline and regulatory context; clinicians explain applicable criteria as part of the shared decision process rather than imposing a universal rule.
Risk assessment also includes a review of concurrent medications and history of gastrointestinal or thyroid disease, as these can influence safety and tolerability. Some therapies have specific contraindications or cautions that may inform whether a patient proceeds with a particular agent. In many clinical encounters, the screening discussion leads to a plan for baseline monitoring parameters and an outline of expected follow-up intervals to reassess safety and response.
Documentation of goals and expectations is often part of the screening conversation. Clinicians may encourage patients to articulate short- and longer-term objectives so progress can be measured relative to those aims. Setting measurable clinical markers and scheduling reassessment points helps frame treatment as an iterative process that may be adjusted over time in response to benefits, side effects, and patient preferences.
Many prescription regimens begin with a low starting dose that is increased incrementally to the target dose, a process intended to improve tolerability. Clinicians commonly explain expected titration schedules and typical timelines for dose escalation. They may also describe usual early adverse effects—often gastrointestinal in nature—and how these symptoms are typically managed through temporary dose pauses, slower titration, or symptomatic measures. These are presented as clinical management strategies rather than guarantees of outcomes.

Follow-up monitoring usually involves scheduled visits to assess tolerability, adherence, and markers of clinical response. Clinicians may check weight, vital signs, and pertinent laboratory values at established intervals. Monitoring can include evaluation for adverse effects and assessment of any necessary medication adjustments. The frequency and type of monitoring are individualized, and clinicians frame follow-up as part of ensuring safety and informing whether continuation, modification, or discontinuation is appropriate.
Managing side effects often focuses on symptom mitigation and patient education. Common considerations include dietary adjustments, hydration, temporary dose alteration, and review of concurrent medications that may exacerbate adverse effects. Clinicians may advise patients to report persistent or severe symptoms and will use that information to determine whether to continue, change, or stop therapy. Such approaches prioritize safety and individualized assessment rather than promising a particular tolerability profile.
Documentation of response over time helps guide ongoing decisions. Clinicians often discuss objective and subjective markers—such as weight trends and functional or quality-of-life measures—to determine whether a chosen approach is meeting the patient’s stated goals. If progress is limited or adverse effects are unacceptable, clinicians typically explore alternative agents or comprehensive care adjustments, using clinical reasoning and evidence summaries to inform next steps.
Cost and coverage may influence treatment discussions, and clinicians often review typical factors that affect access, such as insurance formularies, prior-authorization processes, and out-of-pocket expense variability. These elements can affect the feasibility of a given plan for an individual, so clinicians may present them as practical considerations alongside clinical suitability. Describing common cost-related scenarios helps patients anticipate administrative steps without implying specific financial outcomes.
When preparing to discuss options, patients and clinicians may outline questions about expected monitoring, side-effect profiles, and how treatment fits with other medical conditions. Clinicians commonly suggest documenting current medications, recent lab results, and any prior experiences with weight-management therapies to streamline the conversation. Such preparation is framed as facilitating informed discussion rather than promoting a particular choice.
Access strategies that clinicians might explain include methods for verifying coverage, understanding co-pay structures, and timelines for prior-authorization reviews. While administrative processes vary across payers and regions, clinicians often describe typical patterns to set expectations about timeframes and documentation requirements. These operational details are provided to support logistical planning rather than to direct a specific action.
Finally, clinicians and patients often plan follow-up intervals and success criteria collaboratively before beginning a medication. This planning clarifies when to re-evaluate safety and efficacy and what metrics will indicate continuing or modifying the approach. Framing follow-up as an ongoing assessment helps ensure that decisions are responsive to individual response and changing circumstances rather than framed as one-time commitments.