
Cardiac surgery encompasses a range of operative procedures intended to address structural and functional conditions of the heart. This concept includes traditional open procedures such as coronary artery bypass grafting (CABG) and valve repair or replacement, as well as less invasive and catheter-based approaches that may be used for specific patient profiles. The focus in an overview of common procedures and approaches is to describe the methods, typical clinical contexts, and how teams coordinate care rather than to provide personalized medical guidance.
An overview of cardiac surgical approaches typically covers indications, relative procedure characteristics, procedural steps in broad terms, and frameworks for perioperative care. It may also outline how imaging, anaesthesia, and perfusion technologies integrate with surgical technique. Descriptive discussion of these components can help readers understand the range of procedural options and the kinds of clinical settings in which they often occur, without making outcome claims or offering direct medical advice.

Comparing these approaches, clinicians often weigh trade-offs between exposure and invasiveness. Open procedures like CABG or open valve surgery typically provide direct visualization and access, whereas minimally invasive and transcatheter techniques may reduce incision-related morbidity but can require specialized imaging and device expertise. Choice of approach usually depends on patient anatomy, comorbidities, imaging findings, and institutional experience. Descriptions should therefore emphasize relative characteristics rather than categorical superiority.
Surgical planning commonly integrates diagnostic imaging modalities such as echocardiography, computed tomography, and coronary angiography to clarify anatomy and guide approach selection. Multidisciplinary meetings involving surgeons, cardiologists, anaesthesiologists, and imaging specialists often occur to discuss procedural strategy and risk assessment. Preoperative optimization may focus on stabilizing cardiac status and addressing modifiable factors; explanations of planning processes should remain general and descriptive rather than prescriptive.
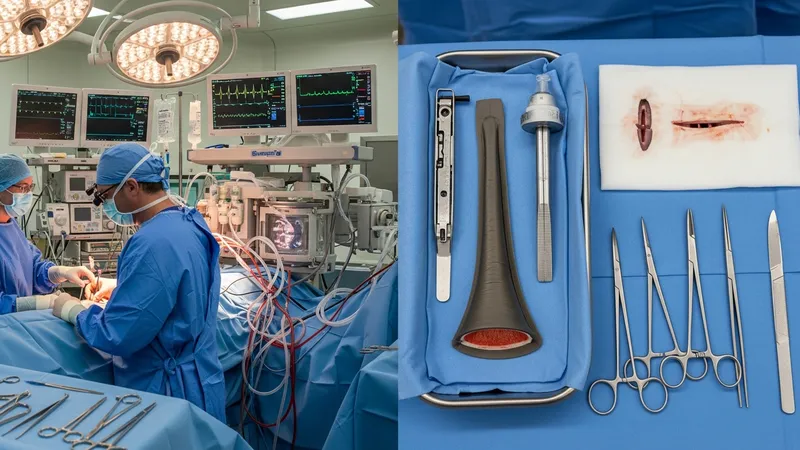
Intraoperative techniques vary by procedure and can include use of cardiopulmonary bypass, off-pump strategies, specialized retractors, and suture or device systems for valve work. Perfusion management and myocardial protection are frequent topics in operative descriptions, with teams using techniques that may include cardioplegia or controlled reperfusion. Describing these intraoperative components in neutral terms helps readers appreciate technical diversity without implying outcome guarantees.
Post-procedural care frameworks typically involve intensive monitoring, pain control, early mobilization, and staged rehabilitation. Hospital length of stay and follow-up schedules vary with procedure type and individual recovery patterns. Rehabilitation and secondary prevention strategies such as risk-factor management may be referenced as part of a continuum of care; such references should be framed as general components of recovery planning rather than medical advice for individuals.
In summary, an overview of cardiac surgery procedures and approaches describes the major procedure types, planning elements, operative techniques, and post-procedural frameworks in measured language. This general exposition aims to clarify commonly described options and considerations without offering prescriptive recommendations. The next sections examine practical components and considerations in more detail.
Common cardiac surgical types include coronary revascularization, valvular surgery, congenital repairs, and procedures to address arrhythmia substrates. Coronary revascularization, often represented by CABG, is typically discussed for multivessel coronary disease when anatomy or clinical context makes surgical grafting appropriate. Valve surgery addresses structural valve disease and may involve repair or replacement depending on valve pathology and tissue quality. Congenital repairs cover a range of anatomical corrections often performed in specialized centers. Descriptions of indications usually present diagnostic criteria and contextual factors rather than prescriptive thresholds.
Indications for different approaches can vary with patient characteristics. For example, minimally invasive or transcatheter options may be considered for patients who have high surgical risk or specific anatomic suitability, whereas more invasive approaches may be selected when extensive exposure is needed. Risk stratification frameworks such as clinical scoring systems are often used to inform discussions, though exact thresholds and decisions typically remain individualized and are usually decided by multidisciplinary teams.
Procedural selection may also reflect institutional capabilities and operator experience. Some centers may routinely offer off-pump CABG or hybrid revascularization strategies that combine surgical and percutaneous techniques, while others may concentrate on conventional on-pump procedures. Descriptive coverage of these patterns can note that availability and local expertise shape which procedures are commonly performed in a given setting, without suggesting universal recommendations.
When describing indications, it is common to reference diagnostic modalities that inform decision-making, including echocardiography for valve assessment and coronary angiography for coronary anatomy. Clinical symptoms, functional testing, and comorbid conditions often factor into procedural choice. Presenting this information as components of a decision framework helps readers understand how types and indications align, using cautious phrasing to avoid implying fixed rules.
Surgical planning typically begins with detailed imaging and physiologic assessment to delineate anatomy and operative risks. Echocardiography commonly provides valve morphology and function data, while coronary angiography maps coronary arterial disease. Computed tomography or cardiac magnetic resonance imaging may be used for structural detail in complex cases. Preoperative assessment often includes evaluation of comorbidities such as pulmonary or renal disease, nutritional status, and functional capacity, all of which can influence approach selection and perioperative goals.
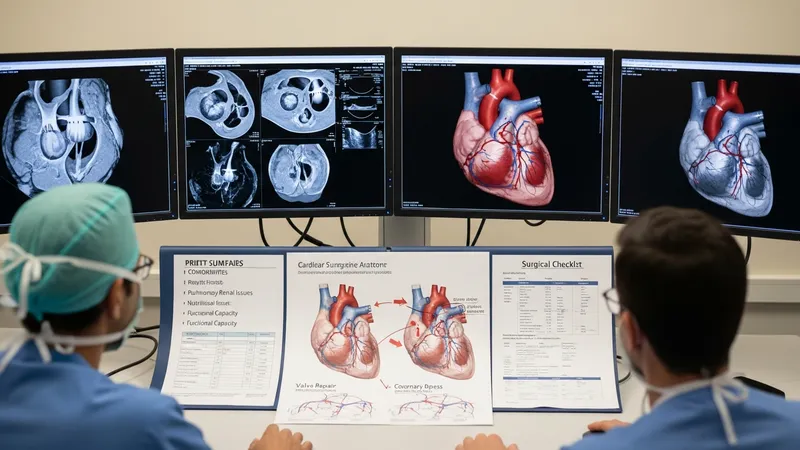
Multidisciplinary case review is a frequent planning element in cardiac surgical practice. Teams that include cardiac surgeons, interventional cardiologists, anaesthesiologists, and imaging specialists may discuss procedural options, potential need for adjunctive technologies, and perioperative resource planning. This collaborative approach often aims to align procedural choice with patient-specific anatomic and clinical factors, though the exact composition of teams and processes can vary between centers.
Preoperative risk mitigation may focus on optimizing reversible conditions and clarifying expectations for recovery. Examples of considerations include adjusting medications, addressing anemia, and planning for organ support strategies if significant comorbidities exist. These are typically described as common considerations rather than directives; the goal in informational material is to outline typical elements of preparation without providing individualized medical instructions.
Imaging and device planning may also be emphasized when minimally invasive or transcatheter procedures are considered. For transcatheter valve procedures, for instance, annular sizing and vascular access assessment are often performed with advanced imaging to determine device suitability. Descriptions of planning steps for these approaches generally highlight that device selection and procedural setup rely on anatomic measurements and team experience.
Operative techniques in cardiac surgery range from full sternotomy access with cardiopulmonary bypass to limited incisions with port-assisted approaches. Cardiopulmonary bypass provides circulatory and respiratory support during many open procedures and involves coordination between surgeon and perfusionist for flow management and myocardial protection. Off-pump techniques attempt coronary grafting on a beating heart to avoid bypass use; descriptions often note the technical demands and patient selection considerations without asserting advantages in all contexts.
Valvular procedures can include reconstructive techniques that preserve native structures or prosthetic replacements that substitute diseased valves. Repair strategies, such as leaflet resection or annuloplasty rings, are described for specific valve pathologies, while replacement options include mechanical or tissue prostheses, each with differing downstream management implications. Such explanations typically clarify method categories and common intraoperative steps rather than suggesting a preferred choice.
Minimally invasive and transcatheter procedures involve distinct intraoperative workflows. Minimally invasive surgery may use smaller thoracotomy incisions and specialized instruments, requiring specific patient positioning and imaging support. Transcatheter approaches rely on catheter navigation and fluoroscopic or echocardiographic guidance to deploy devices via vascular access. Describing these workflows focuses on broad procedural elements and the roles of imaging and device teams rather than providing operational instructions.
Intraoperative monitoring and contingency planning are routinely described as part of safe operative practice. This includes haemodynamic monitoring, readiness for conversion from a minimally invasive to an open approach if necessary, and protocols for managing bleeding or arrhythmia. Presenting these considerations as standard planning components provides readers with a realistic sense of intraoperative complexity without offering procedural advocacy.
Post-procedural care frameworks commonly encompass immediate intensive monitoring followed by stepwise mobilization and discharge planning. Early postoperative monitoring often focuses on haemodynamics, respiratory function, wound status, and pain control. Rehabilitation programs that include graduated activity and cardiovascular risk-factor management are frequently described as components of recovery. These descriptions generally present typical steps in recovery pathways without implying specific timelines for all patients.

Follow-up after cardiac procedures may involve serial imaging to assess graft or valve function, adjustment of long-term medications where indicated, and interventions aimed at secondary prevention of cardiovascular disease. For prosthetic valves, for example, follow-up imaging and consideration of anticoagulation strategies are often discussed in clinical literature; such information should be framed as common clinical considerations rather than individualized recommendations.
Outcomes and recovery trajectories often vary based on procedure type, baseline health, and perioperative events. Educational materials commonly note that recovery timelines may range from days to months and that functional improvement patterns differ across surgery types. Presenting this variability in cautious language helps set realistic expectations without promising particular results or timelines for individual patients.
Long-term surveillance strategies may also address device durability, likelihood of future interventions, and lifestyle or medication adjustments that support cardiovascular health. Descriptions usually emphasize that surveillance protocols are tailored by clinical teams and that periodic assessment is a routine element of care, offering a neutral view of how long-term management commonly unfolds.