
Drug-induced Parkinsonism is a movement disorder that develops as a result of certain medications interfering with dopamine regulation in the brain. Unlike idiopathic Parkinson's disease, which arises spontaneously and progresses chronically, drug-induced forms are typically linked to pharmacological agents that alter neurotransmitter balance. The symptoms closely resemble those of Parkinson's disease, including tremor, muscle rigidity, and slowed movement, but the underlying mechanism is a side effect of medication usage rather than a neurodegenerative process.
This form of Parkinsonism often emerges after exposure to specific classes of drugs, commonly those that affect dopamine receptors or the dopaminergic system. Understanding the origin and triggers of these symptoms is essential for healthcare providers and individuals seeking to differentiate medication-related effects from primary neurological conditions. Accurate identification can support timely reassessment of medication regimens when clinically appropriate.
Drug-induced Parkinsonism typically presents with bilateral symptoms, meaning both sides of the body are affected. This feature may assist clinicians in distinguishing it from primary Parkinson's disease, where symptoms more often begin asymmetrically. The reversibility of symptoms can depend on the medication involved and the individual's response to dose adjustments or discontinuation, although improvement may not be immediate.
Medication classes most frequently implicated are antipsychotics and certain antiemetics, which act by blocking dopamine receptors in the brain. These medications are prescribed for legitimate clinical reasons, such as managing psychiatric disorders or preventing nausea, but the potential for neurological side effects remains an important consideration in ongoing patient care.
Both genetic and non-genetic factors may influence susceptibility to drug-induced Parkinsonism. Age is considered a contributing risk factor, as older adults seem more prone to developing symptoms. Underlying brain changes or coexisting medical conditions might also modify individual risk, even when exposed to the same medication types.
Accurate documentation and monitoring of medication histories play a crucial role in the identification and management of drug-induced movement symptoms. Healthcare professionals often rely on stepwise assessments, including symptom onset timing and specific medication exposures, to evaluate whether mitigating changes to the treatment plan should be explored.
In summary, drug-induced Parkinsonism is a well-recognized consequence of certain medications, notably those influencing dopamine pathways. Distinguishing this condition from idiopathic Parkinson's disease centers on careful evaluation of drug history, symptom patterns, and clinical context. The next sections examine practical components and considerations in more detail.
Antipsychotic medications are among the most commonly associated drugs with the development of parkinsonian symptoms. These medications, such as haloperidol and risperidone, are widely used in the management of psychiatric conditions. Their mechanism often involves dopamine receptor blockade in the central nervous system, which may disrupt normal motor control pathways. Clinicians monitoring individuals receiving these medications frequently assess for emerging movement-related side effects as part of ongoing management.
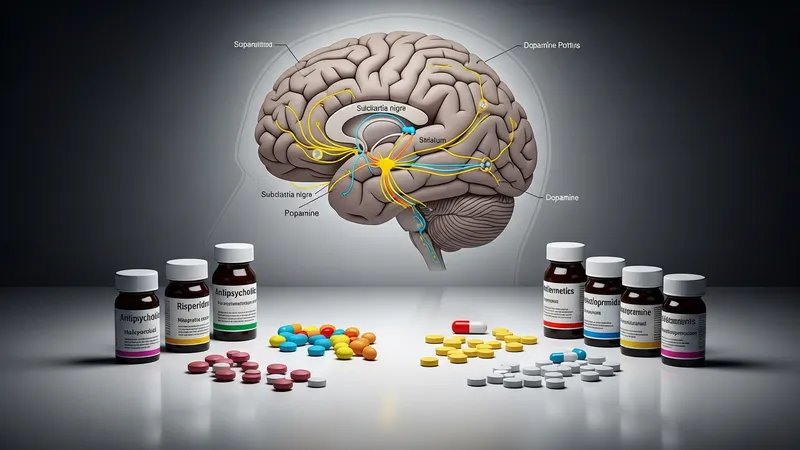
Antiemetic agents, including metoclopramide and prochlorperazine, are frequently prescribed for nausea, vomiting, or gastrointestinal disorders. The pharmacological profile of these drugs includes action on dopamine receptors, which explains their potential to induce parkinsonism in sensitive individuals. While these side effects are relatively uncommon, the association is well-documented in clinical literature and warrants consideration when unexplained motor symptoms present during therapy.
Calcium channel blockers, such as flunarizine, play a role in migraine and hypertension management. Although their primary function relates to vascular regulation, some agents in this class have been reported to produce parkinsonian symptoms, particularly in those with heightened susceptibility. This illustrates how diverse drug classes, beyond standard psychiatric or gastrointestinal medications, may occasionally contribute to movement disorders.
Predicting which individuals may develop drug-induced Parkinsonism remains complex, as not all exposed persons experience symptoms. Factors such as duration of drug exposure, cumulative dose, and intrinsic biological vulnerability can shape risk profiles. Recognizing medication triggers provides an important context for informed diagnostic and therapeutic decision-making. The next page discusses symptom patterns and clinical presentation in greater detail.
The typical symptom profile in drug-induced Parkinsonism includes features such as bradykinesia (slowed movement), rigidity, and resting tremor. A distinctive aspect of this presentation is the frequent bilateral involvement, which contrasts with the more often unilateral onset of idiopathic Parkinson’s disease. Individuals may notice difficulty with fine motor tasks, changes in gait, or generalized slowness, with the timeline of onset often closely linked to the start or dose increase of a causative medication.

Diagnosis relies heavily on a detailed medical and medication history. Clinicians frequently perform a structured review of all recent and ongoing prescriptions, alongside a timeline correlating symptom emergence with medication changes. Physical examination findings, such as decreased arm swing or facial expression, may reinforce suspicions of drug-induced causes, particularly when classical features are present without other neurological findings.
Laboratory and imaging studies are typically used to rule out other conditions but may not demonstrate specific abnormalities in drug-induced Parkinsonism. Diagnostic confirmation often depends on improvement of symptoms following medication dose reduction or withdrawal, which may be guided by safety and psychiatric stability considerations. Persistence of symptoms even after cessation of the causative drug can occur in a subset of cases, often influenced by duration of exposure or preexisting vulnerabilities.
Distinguishing drug-induced from idiopathic forms supports more tailored care and medication management strategies. Recognizing the constellation of clinical features and maintaining awareness of drug-exposure history are key steps in the diagnostic process. The following page addresses risk factors and vulnerability within different population groups.
Age is consistently identified as a leading risk factor for drug-induced Parkinsonism. Older adults appear more susceptible, potentially due to age-associated changes in dopamine systems or pharmacokinetic variables that affect medication clearance. The risk may also be compounded by higher rates of polypharmacy among elderly populations, increasing the likelihood of exposure to drugs associated with parkinsonian side effects.
Genetic factors and underlying medical conditions can also modulate individual vulnerability. Studies suggest that persons with certain genetic backgrounds or those with subclinical changes in the nigrostriatal system may have an increased propensity for developing parkinsonian symptoms when exposed to dopamine-antagonist drugs. The presence of other neurological or chronic conditions may further influence risk, although mechanisms remain under investigation.
The duration and dosage of medication exposure are practical considerations in risk assessment. Longer-term use or higher dosages of implicated drugs, such as antipsychotics and antiemetics, are associated with a greater likelihood of symptom development, although the threshold for individual sensitivity varies. Periodic review of medication necessity and dosage may be part of routine monitoring in at-risk populations.
Polypharmacy and drug interactions represent another layer of complexity. The simultaneous use of multiple medications that influence dopamine regulation can potentially heighten risk, especially in populations managing multiple chronic conditions. Thorough medication reconciliation and awareness of pharmacological profiles are important safeguards in clinical practice. The final page provides an overview of approaches in monitoring and ongoing assessment.
Ongoing assessment of individuals on medications with known associations to parkinsonian symptoms is a fundamental aspect of clinical care. Regular monitoring may include systematic evaluation of motor function, coordination, and gait, in addition to open dialogue about emerging symptoms. These assessments can facilitate early detection of drug-induced changes and inform collaborative decision-making regarding potential medication adjustments.

Documentation of new motor symptoms in conjunction with a detailed review of current and recent medications allows for timely identification of temporal associations. Healthcare professionals may collaborate across specialties to determine if modification of pharmacotherapy is appropriate, while balancing the therapeutic benefits of the implicated drug with the individual's needs and preferences. The process typically involves careful consideration of alternative treatments and risk-benefit analyses.
Education for both clinicians and individuals using at-risk medications plays a role in recognizing early signs of drug-induced movement disorders. Providing factual information on which drugs are most commonly involved, as well as symptom profiles to watch for, can improve prompt reporting and intervention. Updated clinical guidelines and safety communications from authoritative sources support evidence-based practice in this area.
Drug-induced Parkinsonism is widely recognized as a possible side effect of certain medications. Its identification relies on a combination of symptom awareness, meticulous history-taking, and regular monitoring strategies. A well-structured approach may assist in balancing effective medical management with the mitigation of adverse effects within diverse clinical contexts.